Notes
Introduction :
Nitrogenous waste materials in animals are produced through metabolic reactions like anabolism and catabolism. If left to accumulate, they can become toxic and require elimination.
Excretion is closely linked to osmoregulation, which maintains body fluid concentration, and is essential for maintaining homeostasis, which is a steady state required for normal life processes.
Excretion :
The removal of all toxic nitrogenous waste generated by various metabolic process in the body is called as excretion.
- Ammonia, urea and uric acid are the major forms of nitrogenous wastes excreted by animals.
- Apart from nitrogenous wastes, other products like CO2, H2O, bile pigment, etc. also forms the excretory wastes. Such wastes are called as non-nitrogenous wastes.
Excretory Products :
Excretion product and their modes of excretion are described below.
Three main modes of excretion in animals :
(i) Ammonotelism :
- Elimination of nitrogenous wastes in the form of ammonia is called as ammonotelism.
- Ammonia is basic in nature and hence it can disturb the pH of the body, if not eliminated immediately.
- Any change ‘in pH would disturb all enzyme catalyzed reactions in the body and would also make the plasma membrane unstable.
- Ammonia is readily soluble in water and needs large quantity of water to dilute and reduce its toxicity.
- This is however an energy saving mechanism of excretion and hence all animals that have plenty of water available for dilution of ammonia, excrete nitrogenous wastes in the form of ammonia.
- Tadpole (larval stage of life cycle of amphibian) is aquatic. Hence, amphibian tadpole can afford to be ammonotelic.
- Animals that follow this mode of excretion are known as ammonotelic animals.
- 1 gm ammonia needs about 300 — 500 ml of water for elimination.
- Ammonotelic animals excrete ammonia through general body surface (skin), gills and kidneys.
- Ammonotelism is found in aquatic invertebrates, bony fishes, and aquatic / larval amphibians.
- Animals without excretory system (Protozoa) are also ammonotelic.
(ii) Ureotelism :
- The main nitrogenous waste is urea (H2N-CO-NH2).
- Animals excreting urea as nitrogenous wastes are ureotelic.
- It is a common method of excretion in human, whales, seals, camels, kangaroo, toads, frogs, sharks, etc. These animals convert urea in liver by operating ornithine/urea cycle (Krebs and Hanseleit, 1932).
- Three ATP molecules are used to produce one molecule of urea.
- Urea is less toxic and easily soluble component.
- It takes about 50 mL H2O for removal of 1 g NH2 in form of urea.
- Some animals secreting ammonia as waste can be ureotelic also. It is also called double excretion, e.g. earthworm, frog, lung fish, etc.
(iii) Uricotelism :
- Elimination of nitrogenous wastes in the form of uric acid is called as uricotelism.
- Uric acid is least toxic and hence, it can be retained in the body for some time in concentrated form.
- It is least soluble in water. Hence there is minimum (about 5-10 ml for 1 gm) or no need of water for its elimination.
- Those animals which need to conserve more water follow uricotelism. However, these animals need to spend more energy.
- Ammonia is converted into uric acid by ‘inosinic acid pathway’ in the liver of birds. e.g. Birds, some insects, many reptiles, land snails, are uricotelic.
- This mode of excretion can also help reduce body weight (for flight) and those animals which need to conserve more water follow uricotelism.
- Hence, in order to conserve water as an adaptation for flight, birds are uricotelic in nature.
- Animals secrete wastes in form of solid or semi-solid uric acid and are called uricotelic.
Guanotelic Animals : Animals like spiders, scorpions and penguins are guanotelic organisms as they excrete guanine.
Guanotelism :
Guanine is the byproduct of nucleotide metabolism. It is excreted in semi-solid form in spiders, scorpions and penguins. This mode of excretion is called guanotelism.
| Know This :
Creatinine is excreted via urine. Its concentration is interpreted as a measure of the Glomerular Filtrate Rate (GFR) and is thus, used as an index of kidney function. |
Osmoregulation :
- It refers to regulation and maintenance of constant osmotic and ionic concentration of the body fluids.
- Kidneys are important regulators of the body's salt and water requirement. Osmoregulation is homeostasis of the body, i.e. the maintenance of constant internal environment of the body.
- An important role is played by excretory organs by the osmoregulation. Many organisms have special glands for it.
- In animals, this process is brought about by osmoreceptors, which can detect change in osmotic pressure.
- Humans and most other warm-blooded organisms have osmoreceptors in the hypothalamus.
- Animals can either be isoosmotic to the surrounding (osmoconformers) or control internal environment independent of external environment (osmoregulators).
On the basis of an organism's osmoreception property, they are classified as
- Osmoconformers : These organisms maintain the same osmotic pressure inside the body as their outside environment, e.g. starfish, jellyfish, lobsters, etc.
- Osmoregulators : These organisms actively regulate their osmotic pressure independent of the surrounding environment, e.g. freshwater fishes, humans, etc.
Excretory Organs in Different Animals :
- Unicellular organisms have contractile vacuoles which collect and discharge waste products outside the cell.
- Excretion in sponges takes place by diffusion of waste material in water. This waste is discharged through the osculum.
- True organs of excretion are found in those animals that show bilateral symmetry.
- The most common type of excretory organ is a simple or branching tube that opens to the exterior, through pores called nephridiopores. This system is generally found in some annelids, Amphioxus, earthworms, etc.
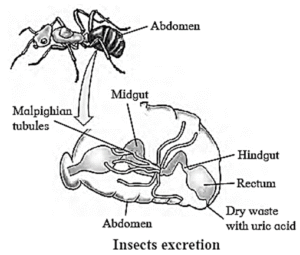
- In most of the insects, excretion takes place by a set of blind ended tubules called malpighian tubules.
- Crustaceans have green glands as excretory organs.
- Members of phylum Echinodermata do not have any specialised excretory organs. Waste materials directly diffuse into water or are excreted through tube feet.
- As we see excretion in lower to higher animals, their excretion process varies like in sponges, it occurs through osculum by diffusion process and in most advanced mammals, it occurs via well-developed kidneys.
- The mammalian kidneys are a collection of functional units called nephrons, which are well designed to excrete metabolic waste.
Excretory organs :
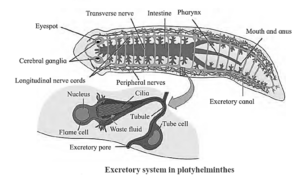
- Protonephridia or Flame cells : They are the excretory structures in Platyhelminthes (e.g. Planaria), rotifers, some annelids and the cephalochordate-Amphioxus. They are primarily concerned with ionic and fluid volume regulation, i.e. osmoregulation.
- Metanephridia : They are tubular excretory structures in earthworms and other annelids. It helps to remove nitrogenous wastes and maintain a fluid and ionic balance. Body fluid enters the nephridium through nephrostomes (funnel-like structures) and gets discharged through nephridiopore.
- Malpighian tubules : They are the excretory structures of most of the insects including cockroaches and helps in the removal of nitrogenous wastes and osmoregulation.
- Antennal glands or Green glands : They perform the excretory function in crustaceans like prawns.
Human Excretory System :
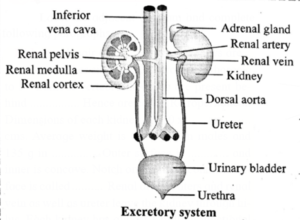
Excretory system of human consists of the following parts
(i) A pair of kidneys.
(ii) A pair of ureters (25-30 cm in length)
(iii) A single unpaired urinary bladder.
(iv) Urethra in males or vestibule in females.
Kidneys : Structure/Morphology :
- These are bean-shaped, chocolate brown structures lying in the abdomen, one on each side of the vertebral column just below the diaphragm.
- The left kidney is placed a little higher than the right kidney (but reverse in rabbit).
- The positioning of kidney is called retroperitoneal, i.e. located outside the peritoneal cavity.
- An average size of kidney is about 10-12 cm in length, 5-7 cm in width and 3-4 cm in thickness. Their weight is about 150 g in males and about 135 g in females.
- Concavity (form of deep notch) of kidney called hilum. These form the urine and control osmotic pressure within the organism with respect to external environment.
- It is the region through which the blood supply, i.e. renal artery and renal vein, pass in and out of the kidney along with the ureter and the nerve supply.
Internal Structure of Kidney :
Each kidney is covered by a semi-liquid fatty tissue called adipose capsule.
Outer covering of this capsule is made up of tough fibrous connective tissue called renal fascia.
Each kidney has three layers of tissue covering it: the outermost renal fascia, the middle adipose capsule, and the innermost renal capsule.
- The renal fascia, the outermost layer, is composed of a thin layer of fibrous connective tissue.
- The middle layer is a mass of fatty tissue called the adipose capsule, which attaches the kidney to the abdominal wall and surrounding tissue. It protects the kidneys by absorbing shock.
- The innermost layer, the renal capsule, is a smooth, translucent fibrous membrane that connects to the ureters' outer layer. It serves as a barrier to the transmission of infections in the kidney.
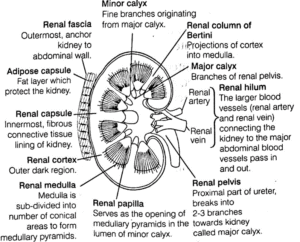
The L.S, of kidney shows two distinct regions within the capsule. Histologically, kidney is divisible into two regions as renal cortex and renal medulla.
- Renal cortex : The outer covering of kidney is called as renal capsule. It is a covering of fibrous connective tissue that protects kidney from injuries and infections. The layer of renal fascia helps the kidneys attach to body wall. It also helps in protection.
- The medulla : It is divided into few concial masses called medullary pyramids, which projects into calyces (sing. calyx). Each medullary (or renal) pyramid have a broad base towards the cortex and a narrow end towards the pelvis known as renal papilla.
- The extended region of cortex in between the medullary or renal pyramids form renal columns called columns of Bertini.
Nephrons :
- Nephrons are structural and functional units of kidney.
- Each nephron consists of a 4-6 cm long, thin-walled tube called the renal tubule and a bunch of capillaries known as the glomerulus.
- The wall of the renal tubule is made up of a single layer of epithelial cells.
- Its proximal end is wide, blind, cup-like and is called as Bowman’s capsule, whereas the distal end is open.
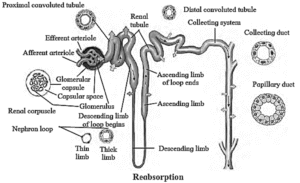
- The nephron is divisible into Bowman’s capsule, neck proximal convoluted tubule (PCT), Loop of Henle (LoH), distal convoluted tubule (DCT) and collecting tubule (CT).
- The glomerulus is present in the cup-like cavity of B0wman’s capsule and both are collectively known as renal corpuscle or Malpighian bodv.
Structure of nephron :
Each nephron is divided into two main parts: (i) Malpighian body (ii) Renal tubule
(A) Malpighian Body or Renal Corpuscle :
It was first observed and described by Marcello Malpighi in 1966. Each Malpighian body is about 200um in diameter and it consists of Bowman's capsule, afferent-arteriol glomerulus and efferent arteriole. It constitute the main part of nephron which filters blood through Glomerular Filtration (GF) and transfer the filtera to the distal part of nephron.
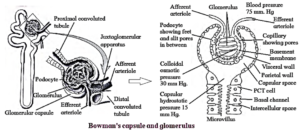
(i) Bowman's capsule :
- It is a double-walled epithelial sac present as the dilated blind end of nephron containing glomerular tuft inside.
- It consists of two layers, i.e. the parietal (outer) layer and the visceral (inner) layer.
- The parietal layer is of single squamous epithelium, which do not function in filtration.
- The cells of visceral layer, undergo extensive modification and convert to podocytes or glomerular ephithelial cells.
- These cells give off a large cytoplasmic processes bearing a large number of pedicel or end feet over them.
(ii) Glomerulus:
- Glomerulus is a bunch of fine blood capillaries located in the cavity of Bowman’s capsule.
- A small terminal branch of the renal artery, called as afferent arteriole enters the cup cavity
- (Bowman capsule) and undergoes extensive fine branching to form network of several capillaries.
- This bunch is called as glomerulus.
- The capillary wall is fenestrated (perforated).
- All capillaries reunite and form an efferent arteriole that leaves the cup cavity.
- The diameter of the afferent arteriole is greater than the efferent arteriole. This creates a high hydrostatic pressure essential for ultrafiltration, in the glomerulus.
(B) Renal Tubule :
It consists of Proximal Convoluted Tubule (PCT), loop of Henle, Distal Convoluted Tubule (DCT) which is further continued to collecting duct. The length of renal tubule is approximately 30-40 mm in length.
The tubules are mainly associated with the process of reabsorption and secretion. The reabsorption is the process of taking back the useful material either from filtrate after filtration or from the coelomic fluid came in by the efforts of peritoneal funnel.
(i) Proximal Convoluted Tubule (PCT) :
- The convoluted portion of the vertebrate nephron lies between Bowman's capsule and the loop of Henle. It is found in the renal cortex.
- It is responsible for reabsorbing (50-60%) of the glomerular ultrafiltrate.
- It is the longest part of the renal tubule, which has simple tall cuboidal epithelium with a brush border (microvilli).
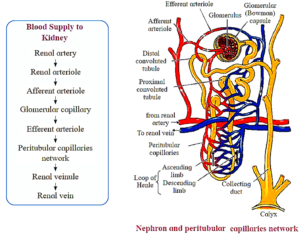
(ii) Henle's loop or Pars recta :
Henle's loop is a U-shaped tube present in medulla, which plays a significant role in maintaining high osmolarity of medullary intestinal fluid.
Loop of Henle is long in mammals and birds, which secrete hypertonic urine, but short in other vertebrates like reptiles, etc.
It is divided into two main segments
- Descending limb : This limb is lined by flat cells, i.e. simple squamous epithelium. It is permeable to water and impermeable to electrolytes. Due to this, the filtrate moving down through the limb becomes concentrated.
- Ascending limb : It is made up of two parts. First is thin ascending limb, lined by squamous epithelium and second thick ascending limb lined by cuboidal epithelium. Ascending limb is impermeable to water, but allows the transport of electrolytes and makes the filtrate dilute.
(iii) Distal convoluted tubule:
- This is another coiled part of the nephron.
- Its wall consists of simple cuboidal epithelium.
- DCT performs tubular secretion / augmentation / active secretion in which, wastes are taken up from surrounding capillaries and secreted into passing urine.
- DCT helps in water reabsorption and regulation of pH of body fluids.
(iv) Collecting duct :
- The last part of nephron is called collecting or straight tubule duct, which is about 20 mm long and lined by the cuboidal cells.
- Several collecting tubules of different nephrons join successively to form the duct of Bellini or papillary duct, which opens at the apex of renal pyramid.
- It reabsorbs the water from the filtrate.
Types of Nephrons
There are two types of nephrons based on difference in their location and functions.
- Cortical nephrons : These nephrons lie in the outer cortex with their short loop of Henle, extending into upper parts of medulla. These constitute 80-85% of total nephrons. They control plasma volume when water supply is normal and vasa recta absent.
- Juxtamedullary nephrons : These nephrons lie at junction of cortex and medulla with their longer loops of Henle, descending deep into the medulla.
- They form 15-20% of total nephrons and control plasma volume, when water supply is short and well developed and vasa recta present.
Ureters:
Structure of Ureters:
- A pair of ureters arise from hilum of each kidney. Each ureter is a long muscular tube 25 — 30 cm in length.
- The wall of ureter is composed of three layers, i.e. external adventitia, middle muscular and inner mucosa. These walls undergo peristalsis to propel the urine from kidneys to urinary bladder.
- Ureters open into urinary bladder by separate openings, which are not guarded by valves.
- They pass obliquely through the wall of urinary bladder. This helps in prevention of backward flow of urine due to compression of ureters while bladder is filled.
Function of Ureters:
- Ureters transport urine from renal pelvis to urinary bladder.
Urinary bladder:
Structure of Urinary bladder:
- It is a median pear-shaped sac. A hollow muscular organ, the bladder is situated in pelvic cavity posterior to pubic symphysis.
- At the base of the urinary bladder there is a small inverted triangular area called Trigone.
- At the apex of this triangle is opening of urethra. At the two points of the base of the triangle are openings of ureters.
- Urinary bladder is covered externally by peritoneum.
- Inner to peritoneum is muscular layer. It is formed by detrusor muscles which consist of three layers of smooth muscles. Longitudinal - circular - longitudinal respectively.
- Innermost layer is made up of transitional epithelial tissue. It helps bladder to stretch.
Function of Urinary bladder :
- Urinary bladder is a temporary storage organ for urine. It helps to expel urine (micturition).
Urethra:
Structure of Urethra:
- It is a fibromuscular tube-like structure arising from urinary bladder and opening to the exterior of the body.
- There are two urethral sphincters between urinary bladder and urethra.
- Internal sphincter: Made up of detrusor muscles, involuntary in nature.
- External sphincter: Made up of striated muscles, voluntary in nature.
- If this valve is not functioning properly during inflammation of bladder, it can lead to kidney infection.
- The urethra in women (4 cm) is much shorter than that of males (20 cm). This allows easy passage of bacteria into the urinary bladder. Hence, urinary tract infections are more common in females than males.
Function of Urethra:
- Urethra is a passage way for discharging urine from body. In males, it acts as urinogenital organ.
Formation of Urine (Uropoiesis) :
Process of urine formation is completed in three successive steps as-
- Ultrafiltration / Glomerular filtration,
- Selective reabsorption,
- Tubular secretion / Augmentation.
Ultrafiltration / Glomerular filtration :
- Diameter of afferent arteriole is greater than the efferent arteriole. The diameter of capillaries is still smaller than both arterioles. Due to the difference in diameter, blood flows with greater pressure through the glomerulus. This is called as glomerular hydrostatic pressure (GHP) and normally, it is about 55 mmHg.
- GHP is opposed by osmotic pressure of blood (normally, about 30 mm Hg) and capsular pressure (normally, about 15 mm Hg).
- Hence net / effective filtration pressure (EFP) is 10 mm Hg.
- EFP = Hydrostatic Pressure in glomerulus — (Osmotic pressure of blood + Filtrate Hydrostatic pressure) = 55- (30 +15) = 10 mm Hg
- Under the effect of high pressure, the thin walls of the capillary become permeable to major components of blood (except blood cells and macromolecules like protein).
- Thus, plasma except proteins oozes out through wall of capillaries.
- About 600 ml blood passes through each kidney per minute.
- The blood (plasma) flowing through kidney (glomeruli) is filtered as glomerular filtrate, at a rate of 125 ml/min. (180 L/d).
- Glomerular filtrate / deproteinized plasma / primary urine is alkaline, contains urea, amino acids, glucose, pigments, and inorganic ions.
- Glomerular filtrate passes through filtration slits into capsular space and then reaches the proximal convoluted tubule.
Selective reabsorption :
- Selective reabsorption occurs in proximal convoluted tubule (PCT). It is highly coiled so that glomerular filtrate passes through it very slowly. Columnar cells of PCT are provided with microvilli due to which absorptive area increases enormously.
- This makes the process of reabsorption very effective.
- These cells perform active (ATP mediated) and passive (simple diffusion) reabsorption.
- Substances with considerable importance (high threshold) like - glucose, amino acids, vitamin C, Ca++, K+, Na+, Cl are absorbed actively, against the concentration gradient. Low threshold substances like water, sulphates, nitrates, etc., are absorbed passively.
- In this way, about 99% of glomerular filtrate is reabsorbed in PCT and DCT.
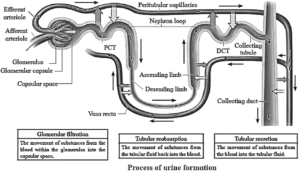
Tubular secretion / Augmentation :
- Finally filtrate reaches the distal convoluted tubule via loop of Henle. Peritubular capillaries surround DCT.
- Cells of distal convoluted tubule and collecting tubule actively absorb the wastes like creatinine and ions like
- K+, H+ from peritubular capillaries and secrete them into the lumen of DCT and CT, thereby augmenting the concentration of urine and changing its pH from alkaline to acidic.
- Secretion of Hl ions in DCT and CT is an important homeostatic mechanism for pH regulation of blood.
- Tubular secretion is the only process of excretion in marine bony fishes and desert amphibians.
Distinguish between Selective reabsorption and Tubular secretion:
| Selective reabsorption | Tubular secretion |
| Selective reabsorption is concerned with the selective absorption of useful substances from the glomerular filtrate. | Tubular secretion is transfer of materials from peritubular capillaries to the renal tubular lumen. |
| Substances with considerable importance (high threshold) like - glucose, amino acids, vitamin C, Ca++, K+, Na+, Cl are absorbed actively, against concentration gradient | In this process, substances like urea, amino acids, glucose, pigments, and inorganic ions are removed from the blood and discharged along with the urine. |
| Selective reabsorption occurs in Proximal convoluted tubule, Henle’s loop, Distal convoluted tubule and collecting duct. | Tubular secretion occurs in Distal convoluted tubules only. |
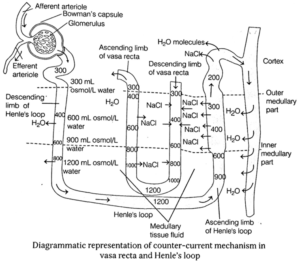
Counter-Current Mechanism of Urine Concentration :
- Mammals produce hypertonic (concentrated) urine due to the presence of counter-current system. This system changes isotonic filtrate to hypertonic urine.
- The longer is the loop of Henle in the nephron, the greater is the ability of an animal to form hypertonic urine.
- The loop of Henle along with blood vessels called vasa recta passes from corticomedullary junction to the medulla and again returns towards the cortex thus, making a hairpin counter-current arrangement.
- The glomerular filtrate enters into the descending limb of Henle's loop in an isotonic state. There is a passive diffusion of Na+ into the tubule from the surrounding hypertonic tissue fluid. Due to such movement of Na+ ions, the tubular fluid becomes
- This hypertonic fluid becomes hypotonic gradually within the ascending limb-due to active transport of Na+ ion from the surrounding and also due to impermeability of wall of this portion to water.
- This hypotonic fluid becomes isotonic gradually again due to the action of ADH after its entry into DCT. This isotonic fluid becomes hypertonic, while passing through the collecting tubule due to ionic and water exchange between the tubular fluid and medullary tissue fluid (hypertonic). This hypertonic fluid is called urine.
Composition of Urine :
It is pale yellow coloured fluid due to the presence of urochrome pigment. It is slightly acidic (average pH 6.0) in nature and is slightly heavier than water. It has a faint aromatic odour due to urinod.
Organic and inorganic components present in urine are given below,
| Organic | Inorganic |
| Urea | Water |
| Uric acid | Sodium chloride |
| Creatinine | Calcium |
| Glucose | Ammonia |
| Creatine | Potassium |
| Ammonia | Chlorides |
| Amino acids | Phosphates |
| Hippuric acid | Magnesium |
Micturition :
- Micturition is the act of voiding the urine.
- The release of urine occurs by the contraction of smooth muscles of urinary bladder wall (due to the pressure exerted by pressure receptors present on the wall) and relaxation of the urethral muscle sphincter around the opening of bladder.
- The urinary bladder acts as a reservoir of urine.
- When 300 to 400 mL urine is accumulated in the bladder, the stretch receptors in the bladder wall are stimulated. In infants, this initiates a spinal reflex action which results to micturition.
- Infants up to 2 years of age show lack of voluntary control over micturition. This is because neurons to the external sphincter muscles are not developed.
Hormonal Control of Body Fluids :
- Osmotic pressure of the blood influences many cellular activities, therefore, the amount of H2O in the body fluids must be regulated.
- In case, the volume of body fluids fall below the normal, glomerular filtration slows down due to decrease in blood pressure and filtration pressure in the glomerular capillaries.
- Hypothalamus in midbrain has special receptors called osmoreceptors, which detect change in osmolarity (measure of total number of dissolved particles per litre of solution) of blood.
The figure given below depicts regulation of body fluids by Antidiuretic Hormone (ADH).
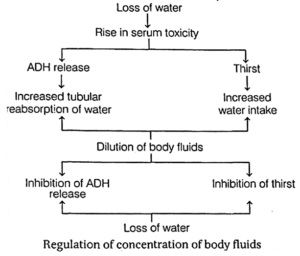
This stimulates the posterior pituitary lobe to release ADH (Antidiuretic Hormone).
(i) Antidiuretic Hormone (ADH) :
- It is secreted by neurohypophysis to control vasopressin increase in osmolarity of blood.
- It increases the reabsorption of water in DCT and collecting duct.
- Less filtration and more reabsorption of water leads to the discharge of small amount of hypertonic urine.
- This raises the volume of body fluids to the normal.
(ii) Aldosterone :
- It is secreted by adrenal cortex and causes reabsorption of Na+ and H2
- It also increase the excretion of K+ and phosphate.
- Reabsorption of Na+ brings about the uptake of an osmotically equivalent amount of water.
- Absorption of sodium and water increases the blood volume and pressure.
(iii) Renin-Angitensin Aldosterone System (RAAS) :
- A reduced blood pressure causes reduced GFR, resulting in release of Renin by Juxta Glomerular (JG) cells.
- Renin converts plasma protein angiotensinogen into angiotensin I and angiotensin II.
- The angiotensin I increases the BP by, constriction of arterioles and increases GFR. Thus, the Renin Angiotensin-Aldosterone System (RAAS) maintains homeostasis.
- Kidneys regulate body fluid osmoregulation by controlling amount of water with the help of the hormone ADH and sodium with the help of aldosterone and proteins by renin and angiotensin.
(iv) Atrial Natriuretic Factor (ANF) :
- It is produced by atria of heart and results in decrease in blood pressure.
- Action of ADH and RAAS leads to increase in blood volume and osmolarity.
- A large increase in blood volume and pressure stimulates atrial wall to produce atrial natriuretic peptide (ANP).
- ANP inhibits Na+ and Cl− reabsorption from collecting ducts inhibits release of renin, reduces aldosterone and ADH release too.
- This leads to a condition called Natriuresis (increased excretion of Na+ in urine) and diuresis.
Disorders of Excretory System :
(i) Renal Calculi (Kidney Stones) :
These are formed in any portion of urinary tract and obstruct urine out flow from the body.
Depending upon the composition renal calculi, these are classified as follows
- Calcium stones : Made up of calcium oxalate stones or calcium phosphate stones.
- Struvite stones : These are formed in response to bacterial infection caused by urea splitting bacteria. These grows quickly to form struvite stones.
- Uric acid stones : These are formed when people don't drink enough water or consume high protein in their diet.
- Cystine stones : It is a type of genetic disorder caused when kidney excrete too much of certain amino acid.
Presence of renal calculi in urinary tract causes pain below rib cage in back and side ways. Hazy, brownish/reddish/ pinkish urine is formed. Frequent urge to pass urine and pain during micturition.
These can be dignosed via uric acid content of blood, colour of urine, X-ray and sonography of kidneys.
(ii) Renal Failure (RF)/Azotemia :
The partial or total inability of kidneys to carryout excretory function is called renal failure or Kidney failure. It is caused by tubular injury, bacterial toxins, inflammation, etc.
It is classified into two types
- Acute Renal Failure (ARF) It is sudden worsening of renal function after severe bleeding. These occurs a sudden decrease in urine output (oliguria-scanty urine), less than 400 mL/day or less than 0.5m/kg/h children. It can be detected by elevated serum creatinine level.
- Chronic Renal Failure (CRF) It is a progressive and irreversible decline in glomerular filtration rate. It is caused due to chronic glomerulonephritis. It can be detected by reduced kidney size and possibility of anaemia.
(iii) Nephritis :
It is inflammation of renal pelvis, calyces and interstitial tissues due to local bacterial infection. Inflammation affects the counter-current mechanism and the victim fails to concentrate urine. Symptoms includes back pain frequent painful urination.
The abnormal functioning of kidney can lead to several other disorders as are given below
Other disorders of excretory system :
- Uremia It occurs due to high concentration of urea in urine. Blood normally contains 0.01 to 0.03% of urea, but if it rises above 0.05% is called uremia. It may lead to kidney failure.
- Cystitis : It is caused by bacterial infection E.coli. leading to inflammation of urinary bladder.
- Glomerulonephritis (Bright's disease) : It is caused by an injury or infection, leading to inflammation of glomeruli and it get engaged with blood containing RBCs and proteins.
- Haematuria : It is a condition which is marked by the presence of blood in urine due to any injury, infection or renal stones.
- Diuresis/Polyuria : Excess urine output, more than 2L/day.
- Oligouria : Decreased urine output, less than 500 mL/day.
- Anuria : Very little or no urine output.
- Gout : A hereditary disorder. Uric level is increased in blood.
- Nephroptesis / Floating Kidney : Kidney moves from its original position.
- Dysuria : Painful urination, sharp burning sensation during urine passage.
- Pyelitis : Untreated cystitis leads to infection in ureters.
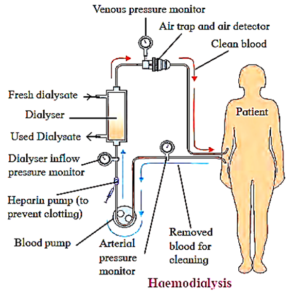
Artificial Kidney/Haemodialyser
Kidney failure can result from infections, injury, or heredity disorders, affecting excretory functions and affecting other organs like the heart.
In cases where kidneys are unfunctionable or damaged beyond repair, artificial kidneys, also known as haemodialysers, are used to filter blood from damaged kidneys, completing the excretory process.
Dr. Belding H Scribner was the inventor of artificial kidney or haemodialyser. Haemodialysis is the separation of small molecules from large molecules in a
solution by interposing a semi-permeable membrane between the solution and water.
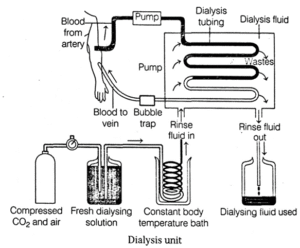
Process of haemodialysis :
- Blood of the patient is pumped from one of the arteries into the cellophane tube after cooling it to 0 0C, generally from the radial artery and passed through a cellophane tube that acts as a semipermeable membrane.
- The tube is immersed in a fluid called dialysate which is isosmotic to normal blood plasma. Hence, only excess salts if present in plasma pass through the cellophane tube into the dialysate.
- Pores of the cellophane tube allow urea, uric acid, creatinine, excess salts, etc., diffuse from the blood into the surrounding solution.
- The blood thus, purified and then is pumped into a vein of the patient. Plasma proteins remain in the blood as the pores of the cellophane are too small to permit the passage of large molecules.
- In this process it is essential that anticoagulant like heparin is added to the blood while it passing through the tube and before resending it into the circulation, adequate amount of anti-heparin is mixed.
Drawbacks of haemodialysis :
- Kidneys are associated with secretion of erythropoietin, renin and calcitriol which is not possible using dialysis machine.
- During dialysis, the blood has to move slowly through the tube and hence the process is slow.
Continuous Ambulatory Peritonial Dialysis (CAPD) :
- A recent development in haemodialysis is the peritoneal dialysis, called CAPD. The peritoneum, semi-permeable membrane of the abdominal cavity is used in dialysis to filter the blood.
- The dialysate fluid moves through permanently inserted catheter into the abdominal cavity of the patients.
- The fluid remains in abdomen and is replaced by new change after several hours (up to 3-4 changes/day).
- Patient is free to move and no connection to any machine is required.
Kidney Transplantation :
Kidney transplant is an organ transplant in a patient with non-functional kidneys or at the end stage of a renal disease.
The organ for transplant procedures can be received from
- a deceased donor (cadaveric)
- a living donor (genetically related or not)
The first cadaveric kidney transplant was done in 1950 in a patient suffering from polycystic kidney disease.
If a person is undergoing kidney transplant, immune suppressants are administered to reduce the occurrence of organ rejection.
Accessory Excretory Organs :
Apart from kidney, some other organs also participates in excretory function. They are not main and essential excretory organs but are called as accessory organs.
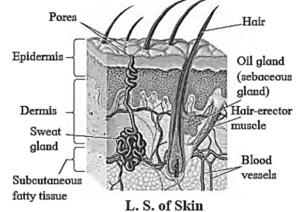
Skin : It helps in removing excess water, salts (NaCl) and other wastes (urea, lactic acid) via sweat and sebaceous gland.
These glands can be described as
(i) Sweat glands :
- These are distributed all over the skin, and are abundant in pain and facial regions. These simple, unbranched, coiled, tubular, glands open on the surface of skin through an opening called sweat pore.
- Sweat is primarily produced for thermoregulation but it also excretes substances like water, NaCl, lactic acid and urea.
(ii) Sebaceous glands :
- These are located at the neck of hair follicles.
- They secrete oily substance skin called sebum. It forms a lubricating layer on sin making it softer.
- It protects skin from infection and injury.
- Lungs : It helps in removing CO2 and little amount of water vapour which are produced during oxidation of food in the cells. About 18 L/hour of CO2 and major quantities of water are removed by lungs everyday.
- Liver : It is the site of formation of major nitrogenous waste in human, i.e. urea which is removed through kidney. Degradation of worn out RBCs into bile pigments also occur here. It also excrete cholesterol, many drugs, some vitamins and major drugs, which are carried by bile to intestine and are passed out with faeces.
- Intestine : The epithelial cells of colon excrete excess of iron, calcium and magnesium along with faeces.
We reply to valid query.